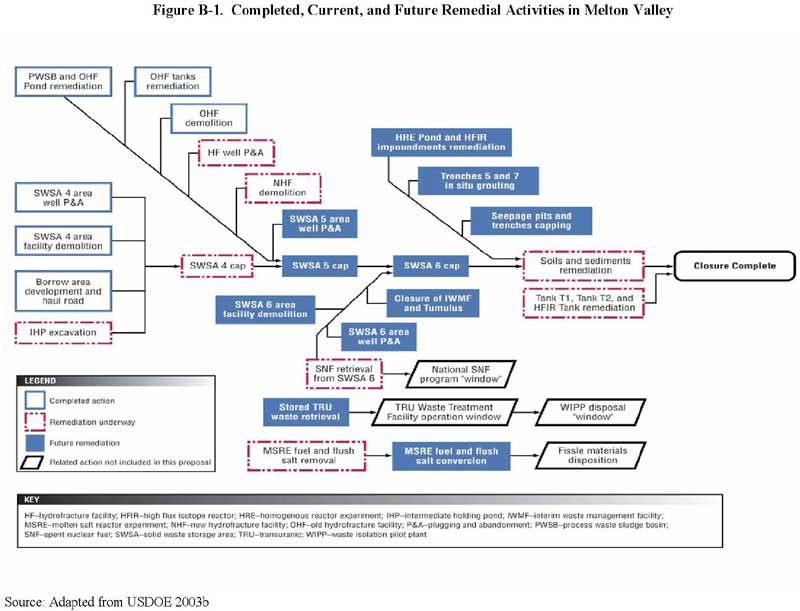
Figure B-1. Completed, Current, and Future Remedial Activities in Melton Valley
Bethel Valley Watershed
The major operations at X-10 take place within the Bethel Valley Watershed. The main plant, key research facilities, primary administrative offices, as well as various forms of waste sites, are situated in Bethel Valley. Over the past 60 years, X-10 releases have contaminated the Bethel Valley Watershed. Mobile contaminants primarily leave the Bethel Valley Watershed via White Oak Creek. These contaminants travel from the Bethel Valley Watershed to the Melton Valley Watershed, where further contaminants enter White Oak Creek. Then, the contaminants that have been discharged to White Oak Creek are released over White Oak Dam and into the Clinch River (USDOE 2001b). The main remedial activities conducted in Bethel Valley are listed below. Please see Figure 10 in Section II.C.1. for a map of Bethel Valley that includes these areas.
See Figures 3 and 10 for the location of First Creek and the Northwest Tributary. In addition, based on suggestions from the 1997 remediation effectiveness report (RER), monthly composite samples are taken at this area, as well as at the Corehole 8 sump (SAIC 2002).
Surface water monitoring in October 1997 revealed elevated levels of Sr 90 and uranium 233 (U 233) in First Creek. In December 1997, further investigation indicated that this contamination was entering the area through two unlined storm drain manholes. As a result, in March 1998, DOE established another interceptor trench that linked to one of the plume's collection sumps. An addendum to the original action memorandum was approved in September 1999. This addendum, which was intended to increase the effectiveness of the initial remedial action, endorsed more groundwater extraction and treatment activities at the Corehole 8 Plume (SAIC 2002). Composite samples are collected monthly at the First Creek Weir, located above First Creek's confluence with the Northwest Tributary, and at the Corehole 8 sump (SAIC 2004). From spring 1995 through fiscal year 2004, the groundwater collection and transmission system reduced fluxes of Sr 90 within First Creek by more than 80% (SAIC 2005).
In September 1997, an Interim Record of Decision (IROD) was signed (SAIC 2002; USDOE 2001c). DOE identified the GAAT cleanup as a priority because of the amount of radiation associated with the tanks, the decaying composition of the tanks, and the considerable risk to X-10 workers and to the environment if a tank leaked or collapsed (USDOE 2001c). The interim action transferred approximately 87,000 gallons of transuranic mixed waste sludge from the GAAT to the Melton Valley Storage Tanks (MVST). The transferred waste was to be treated in the MVST and then shipped to DOE's Waste Isolation Pilot Plant in New Mexico for disposal. This interim action, which removed more than 78,000 curies of waste from the tanks (95% of the contamination), was completed in September 2000. The empty tanks were left in place and grouted (i.e., sealing off the flow of contaminants by pumping cement grout or chemicals into drill holes) in 2001; the remedial action report was approved in October 2001 (SAIC 2002, 2005; USDOE 2001c).
In September 1999, an addendum to this action memorandum added 13 tanks to the original removal action (for a total of 24 tanks), but required the same remedial activities as those specified for the initial 11 tanks. The two-phase removal action was finished in September 2001. Once the tanks were emptied, they were filled with grout and stabilized (SAIC 2002, 2005). In October 2001, a removal action report was approved for the first phase of the removal action. As of fiscal year 2005, the action report for the second removal phase was still awaiting final approval. No monitoring activities are required for the stabilized tanks (SAIC 2005).
Surface Impoundments Operable Unit. This OU consists of four impoundments—Impoundments A, B, C, and D—located in the south–central part of the X-10 site (SAIC 2002, USDOE 2005). The impoundments were used to hold liquid low-level radioactive wastes, byproducts of material processing and various experiments at X-10. Impoundments A and B were unlined; Impoundments C and D were lined with clay. Consequently, Impoundments A and B contained a total of 4,560 cubic yards of radioactive-contaminated sediments, whereas Impoundments C and D contained a total of only 40 cubic yards of low-level, radioactive-contaminated sediments (SAIC 2002). A Record of Decision signed in September 1997 outlined the necessary remedial actions for the surface impoundments. A two-phase remedial alternative took place at this OU, with the initial remedial action phase conducted from August to September 1998. During this time, more sediment samples were collected at Impoundments C and D, and sediment, soil, and water were removed from the impoundments (C and D) and placed into Impoundment B. Following the removal, fresh soil was placed into the excavated areas (SAIC 2002). In April 1999, the remedial action report was approved for the initial remedial phase of Impoundments C and D (SAIC 2002, 2005).
During the next phase, sediment from Impoundment A was moved to Impoundment B, and the excavated area was filled with new soil (SAIC 2002). The sediment in Impoundment B, which contained sediment from all four impoundments, was pumped to an on-site treatment facility, mixed with cement, and placed into a proper shipping container for disposal. In November and December 2002, about 10% of the solidified waste was transported off site for disposal. In spring and summer 2003, the remaining solidified waste was transported to the on-site Environmental Management Waste Management Facility (EMWMF) for disposal. After the sediments were removed, rock and flowable fill were placed into Impoundment B. In May 2004, the remedial action report for Impoundments A and B was approved. No monitoring or institutional controls are required (SAIC 2005).
As of fiscal year 2004, three projects had begun under the Bethel Valley ROD: the Bethel Valley Groundwater Engineering Study; the T-1, T-2, and HFIR tank remediation; and the Hot Storage Garden remediation. In fiscal year 2004, the majority of fieldwork projects necessary for the Bethel Valley Groundwater Engineering Study were completed. The projects included installing 235 soil push probes and 199 soil gas sample receptors, and conducting groundwater, storm sewer, surface water, outfall, and process waste system sampling. In fiscal year 2005, an estimated 15 groundwater wells and 48 additional soil push probes will be installed (SAIC 2005).
The HFIR tank at the X-10 site holds radioactive resin and sludge containing transuranic elements, while two inactive underground storage tanks—T-1 and T-2—hold a mixture of transuranic ion-exchange sludge and resin. Grout will stabilize and keep the HFIR tank waste in place. The T-1 and T-2 tank wastes were mixed, and the remaining slurry moved to the X-10 site's LLLW system. Ultimately, the transferred slurry will be solidified at the TRU Waste Processing Facility before off-site disposal at the DOE Waste Isolation Pilot Plant in New Mexico. In January 2004, a remedial design report/remedial action work plan was approved. All three tanks will be filled with grout and subsequently closed. The schedule for completion is fiscal year 2005 (SAIC 2005).
The Hot Storage Garden, also known as Building 3597, lies in the central plant area of the X-10 site. Radioactive material was historically stored in the building. As a result, traces of radioactive material remain in the facility's old storage wells. Activities at 5 of the 14 wells have been completed. Remedial activities are expected to continue in fiscal year 2005. Due, however, to residual contamination at the facility, the remaining wells will be sealed until initiation of final cleanup efforts, scheduled for 2009 (SAIC 2005).
Melton Valley Watershed
X-10 disposed of its radioactive wastes (liquid and solid) in Melton Valley, and also operated its experimental facilities within this watershed (USDOE 2002a, 2002b). Discharges from Melton Valley's waste areas have produced secondary contamination sources that include sediment, groundwater, and soil contamination. Furthermore, contaminants that are discharged from Melton Valley travel off the reservation through surface water and flow into the Clinch River (SAIC 2002). As a result, the waste sites in the Melton Valley Watershed "...are the primary contributors to off-site spread of contaminants" from the ORR (USDOE 2002b).
The main remedial activities conducted in Melton Valley are detailed below (SAIC 2002; USDOE 2001d; USEPA 2002a). Please see Figure 12 in Section II.C.2. for a map of Melton Valley that includes these areas. Also, please refer to Figure B-1 for the details concerning the completed, current, and future remediation activities in Melton Valley and see Figure B-2 for the Melton Valley projected closure schedule for the current and future activities (USDOE 2003b). The current schedule was accelerated by 9 years to have all closure activities completed by September 2006 (SAIC 2005; USDOE 2003b).
Since the interim action, a fence with many locked gates has enclosed WAG 13. Several signs are posted to notify people that there is on-site soil contamination and restricted access to the site. In addition, the site undergoes surveillance and maintenance inspections on a quarterly basis (e.g., inspecting gates and fences to ensure they are secure) (SAIC 2002, 2005).
Between June 1991 and April 1992, a removal action was conducted at the site. This action consisted of building a sediment retention structure (SRS) at the mouth of White Oak Creek to retain the sediments in the lower embayment and reduce the off-site movement of sediments to the Watts Bar Reservoir and to the Clinch River (SAIC 2002; USEPA 2002a). In 2001, the RER suggested the discontinuation of regular water level monitoring in the WOCE and in the Clinch River. This suggestion, which was implemented in fiscal year 2002, was based on about 10 years of information showing that the SRS could sustain sediment water coverage and prevent scouring of the WOCE (SAIC 2002, 2005). Though regular water level monitoring has ceased, monthly inspections of the SRS (e.g., checking warning signs, assessing if excessive debris has built up, and visually inspecting for indications of the dam shifting) continue to take place (SAIC 2005).
Figure B-1. Completed, Current, and Future Remedial Activities in Melton Valley
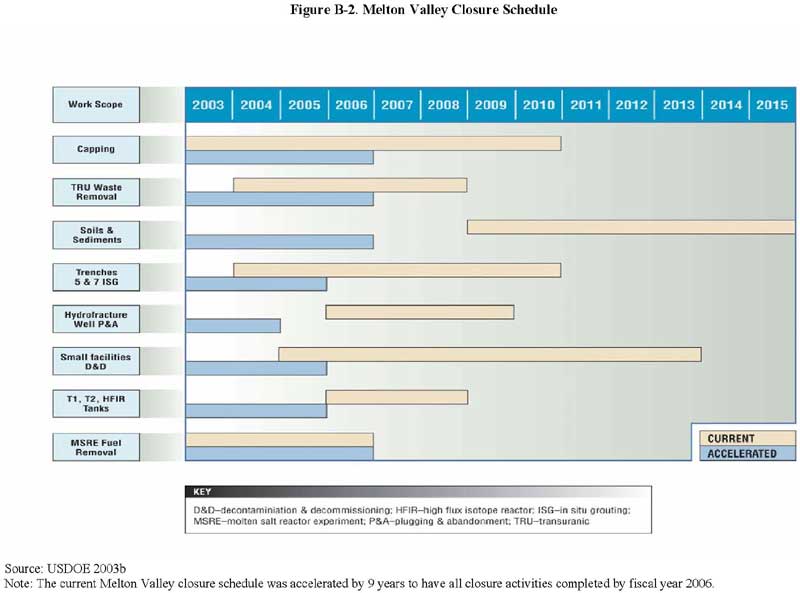
Figure B-2. Melton Valley Closure Schedule
DOE's investigation revealed that two seeps produced about 70% of the overall Sr 90 that was discharged from WAG 4 (SAIC 2002; USDOE 2001e). Because contaminants from these waste trenches migrated into White Oak Creek, grouting techniques were used to reduce the releases of Sr 90 from these trenches; these activities were completed in October 1996. The removal action report, completed in January 1997, identified five monitoring locations at WAG 4 (SAIC 2002; USEPA 2002a). For 5 years, monthly sampling was conducted at these monitoring stations, and as of 2001, the Sr 90 releases had been reduced by about 33% (SAIC 2002). Monitoring was, however, discontinued; it was superseded by a capping project conducted at SWSA 4 under the Melton Valley ROD (SAIC 2005).
According to samples taken in 2000 and 2001, the treatment unit has prevented over 99% of the Sr 90 at Seep C from entering Melton Branch (SAIC 2002). The amount of Sr 90 is greater downstream from Seep C than upstream, which suggests that a portion of the Sr 90 from WAG 5 bypasses the treatment unit (SAIC 2002; USDOE 2001f). In 2002, bimonthly sampling and weekly inspections of the treatment unit at Seep C continued to occur (SAIC 2002). Environmental monitoring of the unit was, however, discontinued in September 2003, and the unit was shut down in fiscal year 2004 (SAIC 2004, 2005). During its operation, the treatment unit at Seep C probably prevented as much as 3 curies of Sr 90 from being released into the Clinch River system (SAIC 2005).
Data collected in 2000 and 2001 showed that this treatment unit has prevented over 99% of the Sr 90 at Seep D from entering Melton Branch (SAIC 2002). However, the amount of Sr 90 is greater downstream at Seep D than upstream. This suggests that small quantities of Sr 90 going into Melton Branch did not originate from the Seep D pumping location (SAIC 2002; USDOE 2001f). Daily inspections are conducted at Seep D and monthly sampling is performed on the treatment unit, as well as upstream and downstream of Melton Branch (SAIC 2002). In addition, as of fiscal year 2004, stream samples were being collected to identify the entry point of Sr 90 into the stream (SAIC 2004). After the first quarter of 2005, the collection system at Seep D will no longer operate. Remedial activities are not expected to include capping of the Seep D area. Nevertheless, the source of releases captured at the Seep D area will be isolated, and the releases will be piped and treated at a new water treatment plant (SAIC 2005).
In May 1999, another OHF-related action memorandum focused on tank stabilization and on the surface impoundment sediments associated with the OHF. The tank stabilization activities identified in the memorandum included removing the piping system, placing submersible pumps into the tanks, using mixer spool pieces, and grouting the tanks. For the surface impoundment, the remedial activities consisted of applying grout for sediment stabilization, placing grout into standpipes, removing excess water, treating any excess water at the PWTP, and using filler material to replenish the impoundment (SAIC 2002). Upon completion of these remedial activities, a May 2001 removal action report was released (SAIC 2002; USEPA 2002a). Under the Melton Valley ROD, the OHF site will be covered by the SWSA 5 cap (SAIC 2005).
In 2004, the ROD was amended to change the proposed treatment remedy at trenches 5 and 7 from in situ vitrification (ISV) to in situ grouting (ISG).17
The Melton Valley ROD remedial activities and their status as of fiscal year 2005 are presented below (ORNL et al. 2004, 2005; SAIC 2002, 2004, 2005; USDOE 2004a, 2004b). Please see Figure 8 for the locations of these areas at X-10 and Figure B-2 for the completion schedule for these activities in Melton Valley.
Summary of ATSDR Activities
Review of clinical information on persons living in or near Oak Ridge. Following a request by William Reid, M.D., ATSDR evaluated the medical histories and clinical data associated with 45 of Dr. Reid's patients. The objective of this review was to assess the clinical data for patients who were tested for heavy metals, and to establish if exposure to metals was related to these patients' various illnesses. ATSDR determined that the case data did not provide sufficient evidence to support an association between these diseases and low levels of metals. The TDOH, which also evaluated the information, reached the same conclusion as did ATSDR. In September 1992, ATSDR provided a copy of its review to Dr. Reid (ATSDR et al. 2000).
Clinical laboratory analysis. In June 1992, William Reid, M.D., an Oak Ridge physician, notified the ORHASP and the TDOH that he believed that about 60 of his patients had been exposed to numerous heavy metals through their occupations or through the environment. Dr. Reid believed that these exposures had caused a number of adverse health outcomes, which included immunosuppression, increased cancer incidence, neurologic diseases, bone marrow damage, chronic fatigue syndrome, autoimmune disease, and abnormal blood clots. Howard Frumkin, M.D., Dr.PH., from the Emory University School of Public Health, requested facilitated clinical laboratory support to evaluate the patients referred by Dr. Reid. As a result of Dr. Frumkin's request, ATSDR and the CDC's NCEH facilitated this laboratory support from 1992 to 1993 through the NCEH Environmental Health Laboratory (ATSDR et al. 2000; ORHASP 1999).
Because of the confidentiality among physicians, as well as the confidentiality between physicians and their patients, the findings of these clinical analyses have not been provided to public health agencies (ATSDR et al. 2000). Nevertheless, in an April 26, 1995, letter to the Commissioner of the Tennessee Department of Health, Dr. Frumkin suggested that one should "not evaluate the patients seen at Emory as if they were a cohort for whom group statistics would be meaningful. This was a self-selected group of patients, most with difficult to answer medical questions (hence their trips to Emory), and cannot in any way be taken to typify the population of Oak Ridge. For that reason, I have consistently urged Dr. Reid, each of the patients, and officials of the CDC and the Tennessee Health Department, not to attempt group analyses of these patients."
Health education. Another essential part of the public health assessment process is designing and implementing activities that promote health and providing information about hazardous substances in the environment.
Coordination with other parties. Since 1992 and continuing to the present, ATSDR has consulted regularly with representatives of other parties involved with the ORR. Specifically, ATSDR has coordinated its efforts with TDOH, TDEC, NCEH, NIOSH, and DOE. These efforts led to the establishment of the Public Health Working Group in 1999, which then led to the establishment of the ORRHES. In addition, ATSDR provided some assistance to TDOH in its study of past public health issues. ATSDR has also obtained and interpreted studies prepared by academic institutions, consulting firms, community groups, and other parties.
Establishment of the ORR Public Health Working Group and the ORRHES. In 1998, under a collaborative effort with the DOE Office of Health Studies, ATSDR and CDC embarked on a process to develop credible, coherent, and coordinated agendas for public health activities and for health studies at each DOE site. In February 1999, ATSDR was given the responsibility to lead the interagency group's efforts to improve communication at the ORR. In cooperation with other agencies, ATSDR established the ORR Public Health Working Group to gather input from local organizations and individuals regarding the creation of a public health forum. After careful consideration of the input gathered from community members, ATSDR and CDC determined that the most appropriate way to meet the needs of the community would be to establish the ORRHES.
Exposure investigations, health consultations, and other scientific evaluations. In addition to the Watts Bar Reservoir, ATSDR health scientists have addressed current public health issues and community health concerns related to other areas affected by ORR operations.
Following are summaries of other ATSDR public health activities involving EFPC:
Summary of U.S. Department of Health and Human Services Activities
U.S. Department of Health and Human Services' evaluation of data in an article from The Tennessean , September 29, 1998. In a November 2, 1998 letter, the Honorable William H. Frist, M.D., United States Senator, requested that Donna E. Shalala, Secretary of the Department of Health and Human Services (DHHS), have the CDC, ATSDR, and the National Institutes of Health (NIH) evaluate the data that the article in The Tennessean describes as reporting a pattern of illnesses among residents living near nuclear plants, including the DOE ORR.
In particular, Senator Frist requested the following:
In a letter dated February 22, 1999, Donna E. Shalala, Secretary of DHHS, responded to Senator Frist's request. DHHS evaluated the article in The Tennessean and responded to Senator Frist's five specific issues. DHHS concluded the following:
Summary of TDOH Activities
Pilot survey. In the fall of 1983, TDOH established an interim soil mercury level to use for making environmental management decisions. CDC evaluated the methodology for this mercury level, and advised the TDOH to conduct a pilot survey to determine if populations with the greatest risk for mercury exposure had elevated mercury body burdens. Between June and July 1984, TDOH and CDC conducted a pilot survey to record the inorganic mercury levels of Oak Ridge residents who had the greatest risk of being exposed to mercury-contaminated fish and soil. In addition, the survey assessed if exposure to mercury through contaminated fish and soil represented an immediate health hazard for the Oak Ridge community. In October 1985, the findings of the pilot study were released; these results indicated that people who lived and worked in Oak Ridge, Tennessee, were unlikely to have a greater risk for significantly high mercury levels. Further, concentrations of mercury detected in hair and urine samples were lower than levels associated with known health effects (ATSDR et al. 2000).
Health statistics review. In June 1992, William Reid, M.D., an Oak Ridge physician, informed the ORHASP and the TDOH that he believed that about 60 of his patients had been exposed to numerous heavy metals through their occupation or through the environment. Dr. Reid felt that these exposures had caused a number of adverse health outcomes that included immunosuppression, increased cancer incidence, neurologic diseases, bone marrow damage, chronic fatigue syndrome, autoimmune disease, and abnormal blood clots. In 1992, TDOH conducted a health statistics review that evaluated the cancer incidence rates for the counties around the reservation between 1988 and 1990, and compared these rates to the state rates for Tennessee. The health statistics review determined that some of the counties' rates were low and some were high when compared to the state's rates; however, the review was unable to distinguish any patterns associated with the site. More detailed findings of the review can be found in a TDOH memorandum dated October 19, 1992, from Mary Layne Van Cleave to Dr. Mary Yarbrough. In addition, the handouts and minutes from Ms. Van Cleave's presentation at the ORHASP meeting on December 14, 1994, are available through TDOH (ATSDR et al. 2000).
Health statistics review. In 1994, area residents reported that there were several community members who had amyotrophic lateral sclerosis (ALS) and multiple sclerosis (MS). TDOH consulted with Peru Thapa, M.D., M.P.H., from the Vanderbilt University School of Medicine, to perform a health statistics review of mortality rates for ALS and MS within certain counties in Tennessee. TDOH also received technical support for the health statistics review from ATSDR (ATSDR et al. 2000).
Because ALS and MS are not reportable, TDOH determined that it was impossible to calculate reliable incidence rates for these diseases. Mortality rates for counties surrounding the ORR were analyzed for the time period between 1980 and 1992, and then compared with mortality rates for the state of Tennessee. The review found that the mortality rates did not differ significantly from the rates in the rest of Tennessee (ATSDR et al. 2000). The following results were reported by TDOH at the ORHASP public meeting on August 18, 1994.
Knowledge, attitudes, and beliefs study. TDOH coordinated a study to evaluate the attitudes, beliefs, and perceptions of residents living in eight counties around Oak Ridge, Tennessee. The purpose of the study was to (1) investigate public perceptions and attitudes about environmental contamination and public health problems related to the ORR, (2) ascertain the public's level of awareness and assessment of the ORHASP, and (3) make recommendations for improving public outreach programs. The report was released in August 1994 (ATSDR et al. 2000; Benson et al. 1994). Following is a summary of the findings (Benson et al. 1994):
Health assessment. The East Tennessee Region of TDOH conducted a health assessment on the eastern region of Tennessee. The purpose of this health assessment was to review the health status of the population, to evaluate the accessibility and utilization of health services, and to develop priorities for resource allocation. The East Tennessee Region released its first edition of A Health Assessment of the East Tennessee Region in December 1991; this edition generally contained data from 1986 to 1990. The second edition, which was released in 1996, generally included data from 1990 to 1995. A copy of the document can be obtained from the East Tennessee Region of TDOH (ATSDR et al. 2000).
Presentation. On February 16, 1995, Dr. Joseph Lyon of the University of Utah gave a TDOH-sponsored presentation at an ORHASP public meeting. The purpose of the presentation was to inform the public and the ORHASP that several studies had been conducted on the fallout from the Nevada Test Site, including the study of thyroid disease and leukemia (ATSDR et al. 2000).
Other Agencies
Assessment reports, environmental studies, health investigations, remedial investigation/ feasibility studies, and sampling validation studies. Other agencies have also addressed community health concerns and public health issues through studies and investigations. Two areas that have been investigated by other agencies—Scarboro and Lower East Fork Poplar Creek (LEFPC)—are discussed below.
Following are summaries of investigations related to the Scarboro community:
In response to this article, on November 20, 1997, the Commissioner of TDOH requested that the CDC assist the TDOH with an investigation of the Scarboro community. TDOH coordinated the Scarboro Community Health Investigation to examine the reported excess of pediatric respiratory illnesses within the Scarboro community. The investigation consisted of a community health survey of parents and guardians, and a follow-up medical examination for children younger than 18 years of age. Both of these components (survey and exam) were essentially designed to measure the rates of common respiratory illnesses among Scarboro children, compare these rates to national rates for pediatric respiratory illnesses, and determine if these illnesses had any unusual characteristics. The investigation was not, however, designed to determine the cause of the illnesses (ATSDR et al. 2000; Johnson et al. 2000).
In 1998, CDC and TDOH were assisted by the Scarboro Community Environmental Justice Oversight Committee to develop a study protocol. After the protocol was created, a community health survey was administered to members of households in the Scarboro neighborhood. The purpose of the survey was to assess if the rates of specific diseases were higher in Scarboro when compared to the rest of the United States, and to determine if exposure to different factors increased the Scarboro residents' risk for health problems. In addition, the survey collected information from adults about their occupations, occupational exposures, and general health concerns. The health investigation survey had an 83% response rate, as 220 out of 264 households were interviewed; this included 119 questionnaires about children and 358 questionnaires about adults in these households (ATSDR et al. 2000; Johnson et al. 2000).
In September 1998, CDC released its initial findings from the survey. For children in Scarboro, the asthma rate was 13%; this was compared to nationally estimated rates of 7% for children between the ages of 0 and 18, and 9% for African American children between the ages of 0 and 18. Still, the Scarboro rate fell within the range of rates (6% to 16%) found in comparable studies across the United States. The wheezing rate was 35% for children in Scarboro, which was compared to international estimates that fell between 1.6% and 36.8%. With the exception of unvented gas stoves, the study did not find any statistically significant link between exposure to typical environmental asthma triggers (e.g., pests, environmental tobacco smoke) or possible occupational exposures (i.e., living with an adult who works at the ORR) and asthma or wheezing illness (ATSDR et al. 2000; Johnson et al. 2000).
After review of information obtained in the health investigation survey, 36 children were invited to have a physical examination; this number included the children who were discussed in the November 1997 newspaper article. In November and December 1998, these medical examinations were conducted to verify the community survey results, to evaluate if the children with respiratory illnesses were receiving necessary medical care, and to confirm if the children detailed in the newspaper actually had those reported respiratory medical problems. The children who were invited to have medical examinations had one or more of the following conditions: 1) severe asthma, which was defined as more than three wheezing episodes or going to an emergency room as a result of these symptoms; 2) severe undiagnosed respiratory illness, which was defined as more than three wheezing episodes and going to an emergency room as a result of these symptoms; 3) respiratory illness and no source for regular medical care; or 4) identified in newspaper reports as having respiratory illness. Out of the 36 children invited, 23 participated in the physical examination. A portion of the eligible children had moved away from Scarboro, whereas others were unavailable or opted not to participate (ATSDR et al. 2000; Johnson et al. 2000).
During the physical examinations, nurses asked the participating children and their parents a series of questions about the health of the children; volunteer physicians evaluated the findings from the nurse interviews and examined the children. In addition to these physical examinations, the children were given blood tests and a special breathing test. The examining physician sometimes took an x-ray of the child, but this was determined on a case-by-case basis. All of the tests, examinations, and transportation to and from the examinations were provided without charge (Johnson et al. 2000).
As soon as the examinations were completed, the results were evaluated to see if any children required immediate intervention, but none of the children needed urgent care. Several laboratory tests revealed levels that were either above or below the normal range, which included blood hemoglobin level, blood calcium level, or breathing test abnormality. After a preliminary review of the findings, laboratory results were conveyed to the parents of the children and their doctors by letter or telephone. If the parents did not want their child's results sent to a physician, then the parents received the results over the telephone. The parents of children who had any health concern identified from the physical examination were sent a personal letter from Paul Erwin, M.D., of the East Tennessee Regional Office of the TDOH, that informed the parents that follow-up was needed with their medical provider. If the children did not have a medical provider, the parents were advised to contact Brenda Vowell, R.N.C., a Public Health Nurse with the East Tennessee Regional Office of the TDOH, for help locating a provider and about possibly receiving TennCare or Children's Special Service (ATSDR et al. 2000; Johnson et al. 2000).
On January 5, 1999, a group of physicians from the CDC, TDOH, the Oak Ridge medical community, and the Morehouse School of Medicine, conducted a thorough review of the findings from the community health survey, the physical examinations, the laboratory tests, and the nurse interviews. From the 23 children who were physically examined, 22 of these children had evidence of some type of respiratory illness, which was discovered during the nurse interviews or during the doctor's physical examinations. Overall, the children seemed to be healthy and no problems requiring immediate assistance were identified. Many of the children had mild respiratory illnesses at the time of their examination, but only one child was found to have a lung abnormality during the examination. In addition, none of the children experienced wheezing at the time of their examination. The examinations did not indicate an unusual illness pattern among children in the Scarboro community. The illnesses that were identified from these examinations were not more severe than would be expected, and they were characteristic of illnesses that could be found in any community. Basically, the results of these examinations validated the results from the community health survey. On January 7, 1999, the results from this team review were presented at a Scarboro community meeting. In July 2000, the final report was released (ATSDR et al. 2000; Johnson et al. 2000).
Three months after the letters had been sent to the parents and to the physicians about the results, efforts were made to telephone the parents of the children who had been examined. Eight of the parents were contacted successfully. Since some of the parents had more than one child who participated in the examination, the questions for the eight parents were applied to 14 children. Despite many attempts on different days, the parents of nine children could not be contacted by telephone (Johnson et al. 2000).
Out of the 14 children whose parents had been contacted, seven of the children had been to a doctor since the examinations. For the most part, the health of the children was about the same. However, since the examinations, one child had been in the hospital because of asthma and another child's asthma medication had been strengthened due to worsening asthma. In addition, several parents reported that their children had nasal allergies, and many parents noted problems with obtaining medicines because of the expense and the lack of coverage by TennCare for the specific medicines. Subsequently, TDOH nurses have helped these parents obtain the needed medicines (Johnson et al. 2000).
The level of radiation was below background levels and the radionuclide analytical values did not indicate a level of health concern. Uranium levels in the core soil samples were also below background levels. EPA concluded that the results support the sampling performed by FAMU in 1998, and that there is not an elevation of chemical, metal, or radionuclides above a regulatory health level of concern. The residents of Scarboro are not currently being exposed to harmful levels of substances from the Y-12 plant. The report stated that "based on EPA's results, the Scarboro community is safe. Therefore, additional sampling to determine current exposure is not warranted." A final report was released in April 2003 (USEPA 2003b).
Following is a summary of a remedial investigation/feasibility study (RI/FS) for LEFPC:
TDOH's Phase I Dose Reconstruction Feasibility Study (PDF, 237KB)
TDOH's Task 4 Radionuclide Releases to the Clinch River From White Oak Creek on the Oak Ridge Reservation (PDF, 246KB)
TDOH's Task 7 Screening Level Evaluation of Additional Potential Materials of Concern (PDF, 200KB)
ATSDR's Health Consultation on the Lower Watts Bar Reservoir (PDF, 176KB)
ATSDR's Watts Bar Exposure Investigation (PDF, 212KB)
TDEC's Watts Bar Reservoir and Clinch River Turtle Sampling Survey (PDF, 208KB)
TDOH's Task 6 Uranium Releases From the Oak Ridge Reservation (PDF, 187KB)
Table E-1. Conservative Screening Indices for Radionuclides in the Clinch River
Isotope |
Exposure Pathway |
||||||||
|---|---|---|---|---|---|---|---|---|---|
| Drinking Water | Fish Ingestion |
External: Shoreline |
Swimming |
External: Dredged Sediment |
Ingestion of Beef |
Ingestion of Milk |
Ingestion of Vegetables |
Irrigation |
|
Cs 137 |
9.2 E-06 |
4.0 E-04 |
8.0 E-03 |
7.6 E-07 |
1.6 E-03 |
5.9 E-03 |
5.7 E-03 |
5.6 E-04 |
3.2 E-08 |
Ru 106 |
7.7 E-05 |
1.7 E-05 |
1.1 E-03 |
5.2 E-06 |
4.5 E-05 |
1.6 E-04 |
4.4 E-07 |
5.8 E-05 |
1.2 E-08 |
Sr 90 |
2.5 E-05 |
3.3 E-05 |
7.1 E-05 |
1.5 E-06 |
9.8 E-06 |
1.7 E-02 |
2.5 E-02 |
6.4 E-03 |
5.1 E-07 |
Co 60 |
2.8 E-06 |
1.9 E-05 |
6.0 E-03 |
1.7 E-07 |
8.5 E-04 |
1.1 E-03 |
7.6 E-04 |
7.5 E-05 |
6.2 E-09 |
Ce 144 |
4.2 E-06 |
2.7 E-06 |
2.1 E-05 |
2.6 E-07 |
7.2 E-08 |
1.1 E-08 |
7.4 E-08 |
3.2 E-07 |
2.2 E-09 |
Zr 95 |
8.1 E-07 |
5.3 E-06 |
1.8 E-04 |
4.3 E-07 |
5.1 E-09 |
8.8 E-11 |
2.7 E-10 |
2.1 E-12 |
3.1 E-12 |
Nb 95 |
4.2 E-07 |
2.7 E-06 |
5.1 E-05 |
2.0 E-07 |
3.1 E-09 |
1.4 E-11 |
9.1 E-11 |
1.4 E-11 |
3.7 E-12 |
I 131 |
4.1 E-05 |
6.7 E-06 |
7.2 E-08 |
4.1 E-06 |
3.2 E-12 |
6.0 E-07 |
3.8 E-05 |
1.1 E-11 |
9.3 E-10 |
U 235 |
1.5 E-07 |
3.2 E-08 |
5.0 E-06 |
9.4 E-09 |
7.8 E-07 |
2.8 E-07 |
2.7 E-07 |
4.6 E-07 |
1.8 E-10 |
U 238 |
1.3 E-07 |
2.9 E-08 |
8.4 E-07 |
8.0 E-09 |
1.4 E-07 |
2.5 E-07 |
2.4 E-07 |
4.2 E-07 |
1.6 E-10 |
Pu 239/240 |
9.8 E-07 |
6.4 E-07 |
1.4 E-07 |
5.9 E-08 |
1.5 E-09 |
3.8 E-07 |
2.8 E-08 |
3.1 E-06 |
2.4 E-10 |
Th 232 |
1.0 E-07 |
2.2 E-07 |
9.2 E-08 |
6.1 E-09 |
2.7 E-09 |
2.0 E-08 |
4.8 E-09 |
1.6 E-07 |
1.2 E-11 |
Am 241 |
1.0 E-07 |
6.7 E-08 |
3.8 E-06 |
6.2 E-09 |
2.0 E-07 |
1.7 E-08 |
1.6 E-08 |
2.8 E-07 |
2.5 E-11 |
Eu 154 |
4.9 E-06 |
5.3 E-06 |
3.6 E-08 |
1.1 E-06 |
5.1 E-09 |
1.3 E-06 |
1.7 E-07 |
1.0 E-06 |
4.4 E-10 |
La 140 |
4.9 E-06 |
2.7 E-06 |
1.0 E-06 |
1.8 E-06 |
2.0 E-09 |
1.1 E-07 |
1.6 E-08 |
7.2 E-12 |
3.9 E-13 |
Pm 147 |
7.4 E-07 |
4.8 E-07 |
2.6 E-08 |
4.4 E-08 |
1.1 E-11 |
1.7 E-08 |
2.8 E-09 |
6.0 E-10 |
3.6 3-11 |
Sm 151 |
2.3 E07 |
1.5 E-06 |
1.3 E-07 |
1.4 E-08 |
3.8 E-10 |
90 E-07 |
1.2 E-07 |
7.5 E-07 |
2.7 E-11 |
Sr 89 |
1.5 E-08 |
1.9 E-08 |
1.2 E-11 |
8.8 E-10 |
1.1 E-13 |
1.4 E-09 |
2.4 E-09 |
3.4 E-11 |
0.0 E+00 |
Ba 140 |
8.6 E-07 |
9.4 E-08 |
5.6 E-07 |
2.8 E-07 |
0.0 E+00 |
1.9 E-09 |
2.3 E-08 |
0.0 E+00 |
5.4 E-12 |
P 32 |
7.8 E-08 |
3.8 E-06 |
2.3 E-12 |
4.7 E-09 |
6.9 E16 |
4.2 E-08 |
3.3 E-13 |
3.3 E-13 |
1.6 E-13 |
Y 91 |
7.0 E-06 |
4.6 E-06 |
3.5 E-07 |
4.2 3-07 |
.3 E-11 |
7.6 E-08 |
2.3 E-08 |
1.1 E-10 |
2.9 E-11 |
Pr 143 |
3.5 E-06 |
2.3 E-06 |
9.6 E-09 |
2.1 E-07 |
1.5 E-12 |
7.6 E-08 |
1.1 E-08 |
8.3 E-12 |
0.0 E+00 |
Nd 147 |
3.1 E-06 |
2.0 E-06 |
1.6 E-06 |
2.7 E-07 |
3.6 E-10 |
6.8 E-08 |
1.0 E-08 |
6.0 E-12 |
0.0 E+00 |
Bold values represent radionuclides for each pathway that were carried into the next iteration of analysis in Task 4.
Screening indices are calculated probabilities of developing cancer.
During the public health assessment process, ATSDR uses radiation doses rather than risk
Public health assessments differ from the U.S. Environmental Protection Agency's (EPA) risk assessments, which evaluate hypothetical risk to determine safe regulatory limits and prioritize sites for cleanup. Typically, ATSDR does not incorporate risk numbers in public health assessments. Nevertheless, in response to public requests to describe the methodology used in this public health assessment to convert doses to risk numbers, ATSDR includes this supplemental risk appendix. By applying the methods described in this appendix, community members can estimate for themselves the theoretical risk from exposure to X-10 radionuclides released to the Clinch River and the Lower Watts Bar Reservoir via White Oak Creek.
Differences between Dose and Risk
Dose, as defined by ATSDR, is the "amount of a substance to which a person may be exposed, usually on a daily basis." For chemicals, dose is often referred to as the "amount of substances(s) per body weight per day" and is the basis for determining levels of exposure that might cause adverse health effects. In the case of radiation, dose is the amount of energy deposited in a specific body mass.
The Society for Risk Analysis defines risk as the "potential for realization of unwanted, adverse consequences to human life, health, property, or the environment; estimation of risk is usually based on the expected value of the conditional probability of the event occurring times the consequence of the event given that it has occurred."18 The EPA defines risk as "a measure of the probability that damage to life, health, property, and/or the environment will occur as a result of a given hazard."19
How Does a Risk Assessment Differ from a Public Health Assessment?
Again, EPA defines a risk assessment as a "qualitative and quantitative evaluation of the risk posed to human health and/or the environment by the actual or potential presence and/or use of specific pollutants." Risk assessments—useful in determining safe regulatory limits and prioritizing sites for cleanup—provide estimates of theoretical risk from possible current or future exposures and consider all contaminated media, regardless of whether exposures are occurring or are likely to occur. Quantitative risk estimates developed using the EPA risk assessment methodology include multiple safety factors and are not intended to predict the incidence of disease or measure the actual health effects in people resulting from hazardous substances at a site. By design, EPA risk estimates are conservative predictions that generally overestimate risk. Risk assessments do not provide a perspective on what the risk estimates mean in the context of the site community and do not measure the actual health effects hazardous substances have on people.
The mathematical formula used to calculate risk estimates assumes a linear (i.e., straight line) response to exposure, even though an actual effect may not be detected in an exposed population. The inability to detect an effect could result from the absence of an effect at lower levels of exposure or because the current epidemiological tools are not sufficient to demonstrate the existence of a very small excess of health effects, such as cancer incidence. The conservative approach to risk assessment, which likely overestimates the true potential impact of exposure, is appropriate for exposure prevention and prioritizing site cleanup. Please see Figure F-1 for examples of different models of low-level radiation effects, including the linear model used by governmental and nongovernmental entities to estimate radiation risks.
ATSDR recognizes that every radiation dose, action, or activity may carry an associated risk. ATSDR uses the public health assessment process to evaluate the public health implications of exposure to environmental contamination and to identify the appropriate public health actions for particular communities. A public health assessment provides conclusions about the level of the health threat (if any) posed by a site, as well as recommendations to stop or reduce exposures. Because of uncertainties regarding exposure conditions and because of adverse effects related to environmental levels of exposure, definitive answers are not possible on whether health effects actually will or will not occur. It is possible, however, for a public health assessment to provide a framework that puts site-specific exposures and the potential for harm in perspective.

Figure F-1. Examples of Different Models of Low-Level Radiation Effects 20
ATSDR uses the public health assessment process to answer site-specific questions for people potentially exposed to hazardous substances:
When answering community members' questions about impacts from past, current, and future exposures, extreme overestimations of possible effects can cause unnecessary fear and worry. Therefore, instead of using mathematical formulas to estimate theoretical harm caused by potential exposures, ATSDR provides the public with answers about health effects associated with exposures based on real observations by physicians, epidemiologists, or toxicologists. Using this information, ATSDR will make necessary recommendations to prevent and to mitigate exposures potentially occurring at levels that have been shown to cause adverse health effects. If, however, exposures were at levels below those associated with adverse health effects, further actions would not be recommend.
For more information on the intentional differences between public health assessments and risk
assessments, please see ATSDR's Public Health Assessment Guidance Manual
(http://www.atsdr.cdc.gov/HAC/PHAManual/toc.html), EPA's Risk Assessment Guidance for
Superfund – Human Health Evaluation Manual (http://cfpub1.epa.gov/superapps/index.cfm/fuseaction/pubs.results/results.cfm ![]() ), and A
Citizen's Guide to Risk Assessments and Public Health Assessments at Contaminated Sites (written jointly by ATSDR and EPA Region IV; see http://www.atsdr.cdc.gov/publications/CitizensGuidetoRiskAssessments.html.
), and A
Citizen's Guide to Risk Assessments and Public Health Assessments at Contaminated Sites (written jointly by ATSDR and EPA Region IV; see http://www.atsdr.cdc.gov/publications/CitizensGuidetoRiskAssessments.html.
Radiation Risks
Radiation risks are derived from many exposure studies that have undergone review by governmental and nongovernmental international groups, including
These reviews assist scientists, legislators, regulators, and others in estimating the risks of cancer and deaths associated with radiological exposures and radiological doses.
In its 1991 Publication 60,21 the ICRP discussed risk in terms of radiation detriment and derived probabilities of developing fatal cancers in various organs as measured by the effective dose. The commission also evaluated organ detriment by deriving tissue weighting factors. The ICRP defines a tissue weighting factor as "The factor by which the equivalent dose in a tissue or organ is weighted to represent the relative contribution of that tissue or organ to the total detriment resulting from uniform irradiation of the body." Thus weighting factors convert an organ dose equivalent to a committed effective dose for the whole body. (See Section III.A.1. in the PHA for more information on tissue weighting factors, organ dose equivalents, and effective doses). These weighting factors are applied to ensure the detriment produced is "broadly the same degree" regardless of the tissue or organ irradiated. As mentioned throughout this White Oak Creek public health assessment, the ICRP has a recommended annual radiation dose limit for the public of 100 millirem (mrem)/year. ICRP continues to state, however, that "The Commission does not yet recommend an annual [radiation] risk limit for individuals."
In 1993, the NCRP published risk estimates designed for radiation protection. The NCRP developed these estimates based on a review of studies from UNSCEAR and the National Academy of Sciences' Committee on Biological Effects of Ionizing Atomic Radiation (BEIR). These studies, which included investigations on radiation effects on the thyroid and the fetus, reported the risks associated with exposure to low doses of ionizing radiation. Given its review, the NCRP estimated the following risks for members of the public exposed to ionizing radiation: a lifetime cancer mortality risk of 0.05 per sievert (Sv) (5%); a hereditary risk of 0.01 per Sv (1%), and a risk of severe mental retardation for fetuses exposed at 8–15 weeks gestational age of 0.04 per Sv (0.4%).22
In 1994, the EPA published its methodology for estimating cancer risks from low-level radiation exposures. These estimates, derived from similar data used by the NCRP in Report 115, incorporated 1980 vital statistics to develop organ-specific risks for a stationary US population.23 In Federal Guidance Report 13, released in 1999, the EPA presented refined risk estimates for low-level radiation exposures to be used for various purposes, such as assessing individual sites and conducting general analysis for rule making. These estimates include risks from numerous radionuclides, routes of exposure, and ages of exposure.24
In 2005, the EPA released draft guidelines for carcinogenic risk assessments that discussed guidance for developing and using risk assessments.25 The EPA stated "where alternative approaches have significant biological support, and no scientific consensus favors a single approach, an assessment may present results using alternative approaches. A nonlinear approach can be used to develop a reference dose or a reference concentration." Thus, the EPA indicates that multiple approaches using linear and nonlinear methods are appropriate if more than one mode of action exists. Also, in an EPA Risk Assessment Task Force report titled An Examination of EPA Risk Assessment Principles and Practices, the agency stated that the "risk estimates are designed to ensure that risks are not underestimated, which means that a risk estimate is the upper bound on the estimated risk." Further, the EPA explicitly stated that the true cancer potency "could be as low as zero."26
In a proposed risk assessment bulletin released in 2006, the US Office of Management and Budget (OMB) issued new technical guidance to improve risk assessments prepared by the federal government.27 The bulletin emphasizes the importance of high-technical-quality risk assessments that present scientific issues in an objective manner. According to the OMB, risk assessments need to describe the basis of every critical assumption and specify how the assumptions affect the risk assessment's main findings. An assessment should also discuss the empirical data that both supports and conflicts with the assumptions. The OMB proposed bulletin stated that these discussions should include "the range of scientific opinions regarding the likelihood of plausible alternate assumptions" and "whenever possible, a quantitative evaluation of reasonable alternative assumptions should be provided. If an assessment combines multiple assumptions, the basis and rationale for combining the assumptions should be clearly explained."
To summarize, many governmental and nongovernmental agencies use a linear approach for estimating radiation risks. This linear approach, called the linear nonthreshold (LNT) model, assumes an inherent risk irrespective of the dose. Although this risk has not been seen to date, various agencies use this approach to set regulatory limits, to develop recommended exposure limits for the public, and to evaluate public health hazards (e.g., ATSDR's radiogenic cancer comparison value of 5,000 mrem over 70 years incorporates the LNT model).
Risk Limits
Table F-1 summarizes the organ-specific risk estimates developed by the ICRP (1991) and the EPA (1994 and 1999). The table expresses the results in units of equivalent (organ) dose, and the totals are expressed in terms of effective (whole-body) dose. For the purposes of this discussion, the dose units of Sv and gray (Gy) are interchangeable. The dose unit of rem is equal to 0.01 Sv or 0.01 Gy.
EPA guidance states that carcinogens should be limited to a risk range of 1 in 10,000 to 1 in 1,000,000 (1 x 10-4 to 1 x 10-6), presumably above background exposure. EPA applies this range in its baseline risk assessments to rank sites relatively (primarily) for cleanup; EPA does not, however, determine the likelihood that health effects might occur. The following risk numbers are calculated when the ICRP risk coefficients presented in Table F-1 (converted to 0.0005 per rem) are multiplied by the background radiation dose of 360 mrem/year (including radon) and ATSDR's radiation screening value of 100 mrem/year (for radiation exposure in excess of background):
Exposure to average background radiation (1.8 in 10,000), which cannot be avoided and to which everyone is exposed, exceeds the EPA risk range. The ATSDR screening value of 100 mrem is, however, equivalent to a risk of 5 in 100,000, which falls near the center of EPA's prescribed risk range.
Table F-1. Summary of Organ-Specific Risk Estimates
Organ |
ICRP* (rem) |
EPA† (rad) |
EPA FGR 13‡ (rad) |
|---|---|---|---|
Bladder |
3E-05 |
2.49E-05 |
2.38E-05 |
Bone marrow |
5E-05 |
4.96E-05 |
5.57E-05 |
Bone surface |
5E-06 |
9.00E-07 |
9.50E-07 |
Breast |
2E-05 |
4.62E-05 |
5.06E-05 |
Colon |
8.5E-05 |
9.82E-05 |
1.04E-04 |
Liver |
1.5E-05 |
1.50E-05 |
1.50E-05 |
Lung |
8.5E-05 |
7.16E-05 |
9.88E-05 |
Esophagus |
3E-05 |
9.00E-06 |
1.17E-05 |
Ovary |
1E-05 |
1.66E-05 |
1.49E-05 |
Skin |
2E-06 |
1.00E-06 |
1.00E-06 |
Stomach |
1.1E-04 |
4.44E-05 |
4.07E-05 |
Thyroid |
8E-06 |
3.20E-06 |
3.24E-06 |
Remainder |
5E-05 |
1.29E-04 |
1.54E-01 |
|
|
|
|
Total (whole body) risk |
5E-4 per rem per year |
5.09E-04 per rad per year |
5.75E-04 per rad per year |
0.1 rem/y (100 mrem/y) |
5.00E-05 per year |
5.09E-05 |
5.75E-05 |
Calculation of Risk for the Oak Ridge Public Health Assessments
As previously discussed at public meetings, ATSDR does not perform risk assessments, nor does it report its findings in terms of risk. Calculating the risks from the doses reported by ATSDR in this PHA, however, only involves one additional step. To calculate the risk, multiply the doses reported by ATSDR by the appropriate organ risk factor from Table F-1, being sure to use consistent units throughout the calculations.
Using the following equation, here are some examples of how to calculate the risk from an estimated radiation dose.
Risk = Annual Dose × Risk Coefficient × Years of Exposure
Examples of Calculating Risks From Estimated Radiation Doses
Whole-body dose
Annual Dose (in rem): 100 mrem per year (0.1 rem)
Risk Coefficient: 0.0005 per rem per year
Years of Exposure: 5 years
Risk = 0.1 × 0.0005 × 5 = 0.00025 (2.5 per 10,000)
This result of 2.5 per 10,000 can then be compared to the estimated risk an individual would receive from typical exposures to background radiation during the same time period:
Risk = 0.36 × 0.0005 × 5 = 0.0009 (9 per 10,000)
Dose to the bone marrow
Annual Dose (in rem): 100 mrem per year (0.1 rem)
Risk Coefficient: 0.00005 per rem per year
Years of Exposure: 5 years
Risk = 0.1 × 0.00005 × 5 = 0.000025 (2.5 per 100,000)
Dose to the thyroid
Annual Dose (in rem): 10,000 mrem per year (10 rem)
Risk Coefficient: 0.000008 per rem per year
Years of Exposure: 5 years
Risk = 10 × 0.000008 × 5 = 0.0004 (4 per 10,000)
Next Section Table of Contents