Evaluate the Evidence to Examine Cancer Effects
This section describes the evaluation for examining cancer effects. This process will help you determine whether cancer effects could be possible at your site for contaminants based on your estimated site-specific cancer risks, as well as for known or suspected carcinogens with no available cancer potency factors (also called cancer risk values) to calculate cancer risks.
ATSDR uses the information gathered from the exposure pathway analyses and exposure estimates to derive a range of cancer risks representing typically and highly exposed groups. The cancer estimate is a lifetime excess risk of cancer given duration and frequency of exposure to the contaminant.
ATSDR uses cancer potency factors, also referred to as cancer risk values (i.e., CSFs and IURs), developed by the EPA (see EPA’s Guidelines for Carcinogen Risk Assessment) and, in general, uses EPA’s quantitative approach for estimating a theoretical risk of cancer in an exposed population. Health assessors will use PHAST to calculate cancer risk for both oral and inhalation exposures. For oral exposures, as shown and discussed in the EPCs and Exposure Calculations section, an EPA oral CSF, expressed as risk per mg chemical per kg body weight per day (mg/kg/day)-1, is multiplied by site-specific dose estimates and includes an exposure factor when exposures are less than a lifetime. For inhalation exposures, IUR, expressed as risk per µg/cubic meter, is multiplied by the chemical concentration in the air, again including an exposure factor for less than lifetime exposures. EPA’s Guidelines for Carcinogen Risk Assessment and EPA’s Integrated Risk Information System (IRIS) provide information and describe the methods used to develop these CSFs and IURs for each carcinogen.
ATSDR calculates the cancer risk for children separately from the cancer risk for adults. When childhood exposure continues into adulthood or if exposure occurs for a lifetime, ATSDR combines the cancer risks for children and adults.
For children exposed to mutagenic carcinogens, ATSDR uses EPA’s age-dependent adjustment factors (ADAFs) for early life exposure (discussed in EPA’s Supplemental Guidance for Assessing Susceptibility from Early-Life Exposure to Carcinogens). This approach, as demonstrated in the EPCs and Exposure Calculations section, captures the additional cancer risk that results from early exposure to chemicals with a mutagenic mode of action (MOA).

Unless directly stated, ATSDR cancer risk estimates for exposure to environmental contaminants do not include the existing background cancer rate in the U.S. population. However, including information about background risk provides perspective on the chemical exposure risk. U.S. cancer incidence rates are available from the CDC’s United States Cancer Statistics and the American Cancer Society’s Cancer Statistics Center.
After calculating the cancer risk, health assessors will need to discuss the types of cancer that might be possible. Health assessors should keep in mind that some cancers might be route specific. This process is aimed at weighing the available evidence—in light of uncertainties—and offering perspective on the plausibility of cancer outcomes under site-specific exposure conditions. Use professional judgment when deciding risk for cancer effects, and ask for toxicological assistance to help with these types of evaluations.
Health assessors should not do the following:
- Conduct a comparison between the cancer effect level (CEL; the lowest dose level observed to produce a significant increase in the incidence of cancer or tumors) and site exposure dose to assess cancer effects.
- This is because cancer risk is a linear response without a threshold and very low doses can still cause an increased risk of cancer.
- One exception to this rule is oral exposure to chloroform where EPA has stated that cytotoxicity is necessary before chloroform will cause cancer from ingestion. EPA has stated that their RfD can be considered protective against cancer from oral exposure. More information about chloroform and cancer is available in IRIS.
- Use a CEL to make a health hazard conclusion.
- This is because you need to know the numerical cancer risk to decide whether exposure could cause a significant cancer risk.
A health assessor might look at the CEL if the risk is very high. The purpose would be to see if the site-specific dose or concentration is at cancer effect levels. When site doses approach or exceed the CEL reported in the Toxicological Profile, you can place greater emphasis on the cancer risk estimate.
When communicating the potential for cancer hazards, be sure to state how strongly associated a contaminant is with cancer outcomes. Using plain language, include the cancer classifications in your evaluation (see PHAST for agency-specific classifications) to qualitatively describe the cancer-causing potential of a particular contaminant. ATSDR’s preference is to use the plain text explanations for the different classification categories instead of using an agency’s alphanumeric designation or abbreviation.
However, for some sites, you may encounter potential contaminants of concern that are suspected or known carcinogens, but they do not have oral CSFs or IURs. In these cases, health assessors need to indicate in their documents that quantitative risk estimates are not possible and provide some context as noted below.
- Include information on how you identified the contaminant as a carcinogen (e.g., NTP, EPA, or IARC cancer classification).
- Include highlights from studies supporting the contaminant being a carcinogen, if warranted.
- Indicate what is known in a qualitative way. Provide a paragraph that explains why EPA has not developed CSFs or IURs based on available data (if known), clearly states uncertainty, and includes other relevant information.
- Consult with a toxicologist if there is information on human or animal exposure doses that caused cancer to see if it is appropriate to compare them to site-specific doses.
The example below uses a fictional scenario to demonstrate some of these concepts for conducting a cancer effects evaluation.
Important: This example is for training purposes only. ATSDR, EPA, and other agencies periodically update their values. Always use the most current values and supporting information in your evaluation.
Let’s revisit the drinking water ingestion example for which you calculated CRs for a mutagenic carcinogen in the EPCs and Exposure Calculations Evaluation. In that example, a family was exposed in their home to contaminated drinking water daily, for an unknown number of years. The water has an EPC of 0.00015 mg/L for 1,2,3-trichloropropane. You do not know the number of residents of the home or their ages.
Because you did not have specific information on the residents, PHAST was run using default exposure groups, which incorporates default body weights and default intake rates, to generate exposure doses. PHAST calculates the CRs for this scenario using the ADAF-adjusted cancer risk formula [i.e., (exposure dose) x (age-specific exposure duration/78 years) x (ADAF)] as shown in the table below. Note that this section discusses CRs generated in PHAST for this specific example. For a discussion on example HQs, refer to the Evaluate the Evidence to Examine Non-Cancer Effects section.
Based on this example scenario, ATSDR would further evaluate the potential for cancer effects because either of the CTE and RME CRs, or both, are greater than 1E-6. Always use professional judgment and consider site-specific scenarios to determine whether evaluating CTE and RME is appropriate.
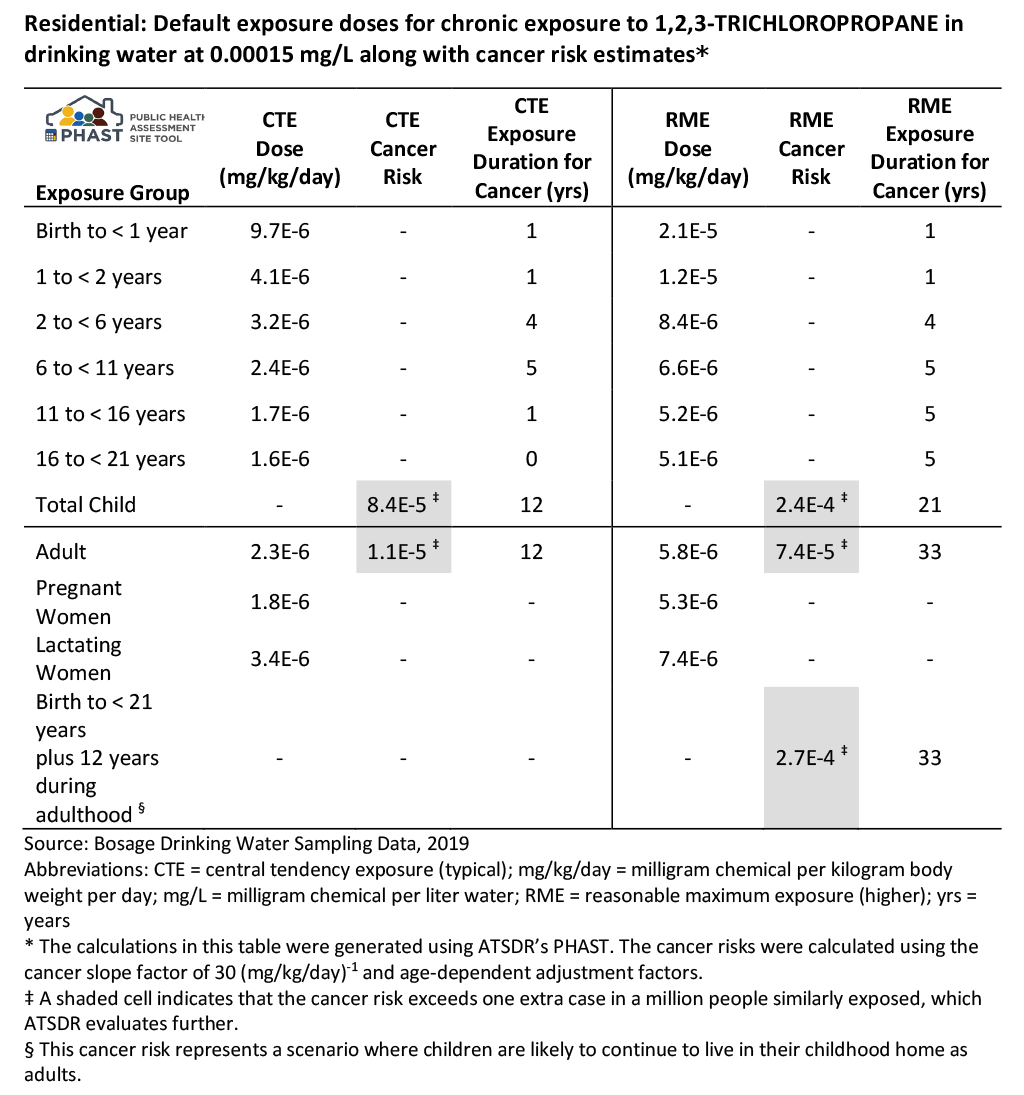
Description of Cancer Example PHAST Results Table
As shown in the table’s footnotes above, PHAST calculated the CRs using EPA’s oral CSF of 30 (mg/kg/day)-1. You can find EPA’s documentation related to developing this cancer risk value (i.e., the CSF) in its IRIS Database.
The table below is a guide for the types of information you might want to gather during the evaluation for cancer, using 1,2,3-trichloropropane as an example. To populate the table for this example exposure scenario for cancer effects, you would use ATSDR’s Toxicological Profile for 1,2,3-Trichloropropane [PDF – 2.4 MB]. You could also refer to the CVs and Health Guidelines Module in PHAST (for the cancer classifications).
Data from Key Studies and Other Information for Cancer Effects: 1,2,3-Trichloropropane
| Parameter | Data for Cancer Effects |
|---|---|
| Cancer risk value | CSF: 30 (mg/kg/day)-1 |
| Information source | EPA IRIS |
| Study reference | NTP. 1993. Toxicology and carcinogenesis studies of 1,2,3-trichloropropane (CAS No. 96-18-4) in F344/N rats and B6C3F1 mice (gavage studies). National Toxicology Program Tech Rep Ser 384. |
| Study exposure route and duration evaluated | Oral, chronic |
| Observed effect for cancer risk value | Tumor types: alimentary system squamous cell neoplasms, liver hepatocellular adenomas or carcinomas, Harderian gland adenomas, uterine/cervix adenomas or carcinomas |
| Species cancer risk value is based on | B6C3F1 mice (female) |
| Dosing method and exposure medium in study | Corn oil by gavage |
| Point of departure (POD) in study |
|
| Mutagenic mode of action (ADA) | Yes |
| Cancer classification(s) |
|
ATSDR uses the cancer classification systems for evaluating contaminant-specific carcinogenicity established by the following agencies: the NTP, the EPA, and the IARC. These agencies classify carcinogens based on the strength of the scientific evidence linking the contaminant with cancer outcomes under the reported conditions of testing. Use these classifications in any discussion of carcinogens. ATSDR may also consider occupational carcinogen classifications by the National Institute for Occupational Safety and Health (NIOSH), if relevant to the exposure scenario being evaluated.
A brief summary of each agency’s cancer classification process is included below. Refer to ATSDR’s Cancer Classification System document for more information.
- NTP completes a hazard assessment of each chemical it evaluates. The hazard assessment examines relevant information on dose response, route of exposure, chemical structure, metabolism, toxicokinetics, sensitive subpopulations, genetic effects, or other data that relate to mode of action or factors that may be unique to a given chemical. Based on a careful review and integration of the body of evidence, NTP classifies the chemical using two cancer classification categories: Known to be a Human Carcinogen and Reasonably Anticipated to be a Human Carcinogen. NTP publishes the findings of its research in its Report on Carcinogens (RoC).
- EPA develops a narrative describing the potential for a chemical’s carcinogenicity, weighing the available evidence and considering any limitations based on dose-rate or dependence on mode of action. EPA emphasizes understanding the mechanism by which a chemical causes cancer to determine whether the mode of action is relevant to humans. This understanding is based on animal findings, risks to sensitive populations or life stages (for which the EPA has issued supplemental guidance), and evaluation of risk assessment options. EPA adopted cancer guidelines in 1986:
- Group A: Carcinogenic to humans
- Group B: Probably carcinogenic to humans (includes B1 and B2)
- Group C: Possibly carcinogenic to humans
- Group D: Not classifiable as to human carcinogenicity
- Group E: Evidence of non-carcinogenicity for humans
EPA revised its guidelines in 2005 but did not reclassify all the chemicals classified under the 1986 EPA guidelines, so it still uses both classification systems. The 2005 classifications are as follows:
-
- Carcinogenic to humans
- Likely to be carcinogenic to humans
- Suggestive evidence of carcinogenic potential
- Inadequate information to assess carcinogenic potential
- Not likely to be carcinogenic to humans
- IARC considers three types of data when evaluating the evidence of chemical carcinogenicity: animal, human, and mechanistic. IARC’s Working Group of expert scientists classifies the animal or human evidence as strong, sufficient, limited, or inadequate. IARC bases its initial categorization on the combined level of evidence from the animal or human data. Strong mechanistic data can provide evidence for raising or lowering the initial category. IARC produces Monographs on the Evaluation of Carcinogenic Risks to Humans, which serve as the basis for IARC cancer classifications:
- Group 1: Carcinogenic to humans
- Group 2A: Probably carcinogenic to humans
- Group 2B: Possibly carcinogenic to humans
- Group 3: Not classifiable as to carcinogenicity to humans
- Group 4: Probably not carcinogenic to humans
- NIOSH determines whether a chemical is an occupational carcinogen by using one of the following three methods:
- Evaluation of chemical carcinogen hazard assessments developed by the
- NTP (“Known to be human carcinogen” or “Reasonably anticipated to be a human carcinogen”)
- EPA (“Carcinogenic to humans,” “likely to be carcinogenic to humans,” “suggestive evidence of carcinogenic potential,” Group A, Group B1, Group B2, or Group C)
- IARC (“Group 1,” “Group 2A,” or “Group 2B”)
- Nomination by NIOSH for classification by NTP
- Classification by NIOSH (described below)
- Evaluation of chemical carcinogen hazard assessments developed by the
NIOSH may perform its own chemical hazard assessment to determine if the chemical should be classified as an occupational carcinogen when the institute has determined that the chemical has the potential for worker exposure and (1) no prior carcinogen classification by NTP, EPA, or IARC has been published or (2) information in the occupational relevance evaluation indicates the need for reconsideration of the evidence underlying a published chemical carcinogen assessment. When developing a new chemical carcinogen classification, NIOSH will use the criteria for carcinogenicity contained in the United Nations’ Globally Harmonized System for Classification and Labelling of Chemicals [PDF – 3.1 MB] (GHS), as included in the Occupational Safety and Health Administration (OSHA) Hazard Communication Standard (29 CFR §1910.1200), and any interpretation of the GHS criteria issued by OSHA. Per NIOSH’s Chemical Carcinogen Policy [PDF – 2.3 MB], if NIOSH determines that the evidence for a chemical corresponds to GHS class 1A, 1B, or 2, and the chemical is occupationally relevant, then the institute will designate the substance an “occupational carcinogen.” (In PHAST, these are labeled with an “OC” designation.)
In general, these agencies draw similar conclusions about carcinogenicity (i.e., their assessment of literature reviews reaches similar conclusions). If the agencies classify a chemical differently, ATSDR usually gives preference to NTP’s classification. However, ATSDR will also consider supporting information that these agencies used to reach their conclusion, particularly if their classifications are based on newer science. Differences between agency classifications may be the result of a more recent literature review and new science or selection of different key studies as the basis for the cancer class designation.
When discussing a chemical’s carcinogenicity, use the plain text explanations for the different classification categories instead of using an agency’s alphanumeric designation or abbreviation. For example, the NTP uses these plain language phrases:
- Known to be a human carcinogen
- Reasonably anticipated to be a human carcinogen
Thus, for a well-documented human carcinogen, the text might read “The National Toxicology Program within the U.S. Department of Health and Human Services has determined that arsenic is known to be a human carcinogen because sufficient evidence exists of carcinogenicity from human studies.” Other examples using plain language phrases are “Human studies clearly link the contaminant of interest with certain cancers” or “While some animal studies have shown increased tumors after exposure to the contaminant of interest, human data do not suggest a link between the contaminant and cancer in humans.”
ATSDR evaluates the relevance of animal data to humans on a case-by-case basis. Without compelling data to the contrary, however, a contaminant that has been shown to cause cancer in animals is considered carcinogenic in humans.
Describing Cancer Risk
In public health documents, ATSDR presents cancer results quantitatively, as a theoretical risk, and qualitatively (see table below). The quantitative results describe the cancer risk numerically, such as three extra cancer cases for every 100,000 similarly exposed persons (3 x 10-5). These theoretical risk estimates are calculated assuming people have the same exposures (e.g., the same soil concentration, soil ingestion rate, specified duration), and do not represent individual cancer risks or account for variation in exposure in people living around a site. For example, a health assessor may use the following type of statement to convey this in a document: Given the conservative nature of the cancer risk evaluation for pentachlorophenol, this cancer risk is not a concern. Note that this is a theoretical estimate of cancer risk that ATSDR uses as a tool for deciding whether public health actions are needed to protect health—it is not an actual estimate of cancer cases in a community.
The objective of the cancer risk estimate (quantitative) and hazard (qualitative) evaluation is to draw conclusions and make recommendations that will protect the public. This table below shows possible recommendations ATSDR may develop for each of the different cancer risk ranges. ATSDR makes recommendations to appropriate parties (e.g., federal, state, and local agencies; community members; tribal governments), which usually focus on these types of primary actions:
- Requesting appropriate parties take steps to stop or reduce the public’s exposure to environmental contaminants
- Educating healthcare professionals about environmental contamination in their communities, including cancer-causing contaminants
- Educating the public about actions which reduce or stop exposures
If state policies are more conservative than the qualitative descriptors in this table below, ATSDR may consider those state policies when summarizing cancer risk. For example, some states are required to designate cancer risks greater than 1 in 1,000,000 (1 x 10-6) as a health concern, while other states may designate 1 in 100,000 (1 x 10-5) as a concern.
ATSDR does not have an acceptable cancer risk range. Therefore, health assessors should do the following:
Health assessors may see theoretical cancer risks written in different ways. For example, the same numerical risk of 1 in 1,000,000 might be written as 1 x 10-6 or as 1E-6.
- Avoid using phrases such as “the estimated cancer risk at this site of two in 100,000 similarly exposed persons is within the acceptable cancer risk range.”
- Avoid stating that the estimated cancer risk is within EPA’s acceptable cancer risk range of 1E-4 to 1E-6. EPA uses this cancer risk range to decide remedial clean-up actions at Superfund sites. ATSDR should not use this range as justification for what is acceptable or not acceptable nor should we report it in our documents.
- Review the following table that describes cancer risk ranges, qualitative descriptors, and possible recommendations.
Quantitative Cancer Risk Range Estimates, Associated Qualitative Descriptors, and Possible Recommendations
| Theoretical Risk Range | Qualitative Descriptor | Possible Recommendations | |
|---|---|---|---|
| ≤ 1E-6 | ≤ 1 in 1,000,000 persons similarly exposed | No concern for increased cancer risk | Usually none |
| > 1E-6 to
< 1E-4 |
> 1 in 1,000,000 to
< 1 in 10,000 persons similarly exposed |
No concern for increased cancer risk*
or A concern for increased cancer risk*
|
If you conclude that there is no concern for increased cancer risk, there are usually no recommendations. However, you could consider public education in ways to reduce exposure or continued monitoring, particularly if the contaminant could migrate and persons could be exposed to higher levels.
If you conclude that there is a concern for increased cancer risk, consider the recommendations below. |
| ≥ 1E-4
|
≥ 1 in 10,000 persons exposed
|
A concern for increased cancer risk | Recommendations that you could consider:
|
*Depends upon your evaluation and whether you decide there is either a concern or not a concern for an increased cancer risk.
This list below presents some issues to consider when deciding whether cancer risks between 1E-6 and 1E-4 are either a concern or not a concern:
- Is the carcinogen a known human carcinogen?
- Are their temporal trends in the data that make you more or less concerned about the calculated cancer risk?
- Are sensitive populations being exposed who might already have an elevated cancer risk?
- Are children exposed early in life, particularly if that exposure involves mutagenic carcinogens?
- Are there data limitations that increase uncertainty (e.g., limited data requiring the use of a maximum concentration as the EPC)?
- Are people exposed to multiple carcinogens as a mixture?
- Is there evidence of a threshold for a specific carcinogen?
- How much does natural background contribute to cancer risk?
- How much does anthropogenic background contribute to cancer risk?
- Are reliable health outcome data (HOD) on cancer rates available for the exposed population?
Before putting the recommended actions for appropriate parties in your site documents, have discussions with these parties to get their input and hopefully their agreement with the recommendations. You may be able to work with these groups on the specific phrasing of recommendations so that they agree to them, making the recommended actions more likely to be done. Identify the agencies for whom the recommendations are intended (e.g., ATSDR, a state environmental agency). And finally, include a discussion about uncertainty in cancer risk estimates along with the quantitative and qualitative description of cancer risk.